Covert Cognition in Disorders of Consciousness: A Meta-Analysis

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
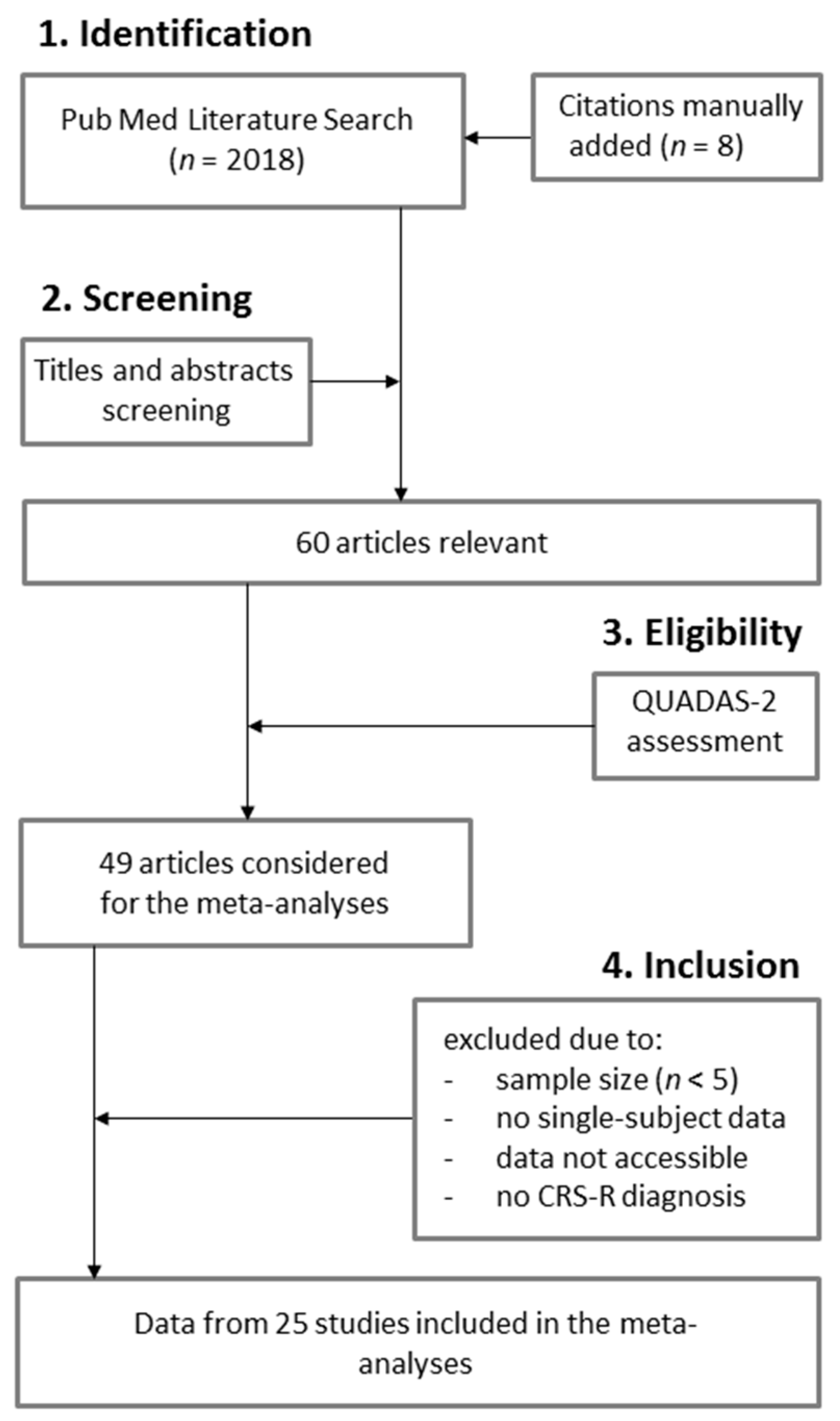
2.2. Search Methods
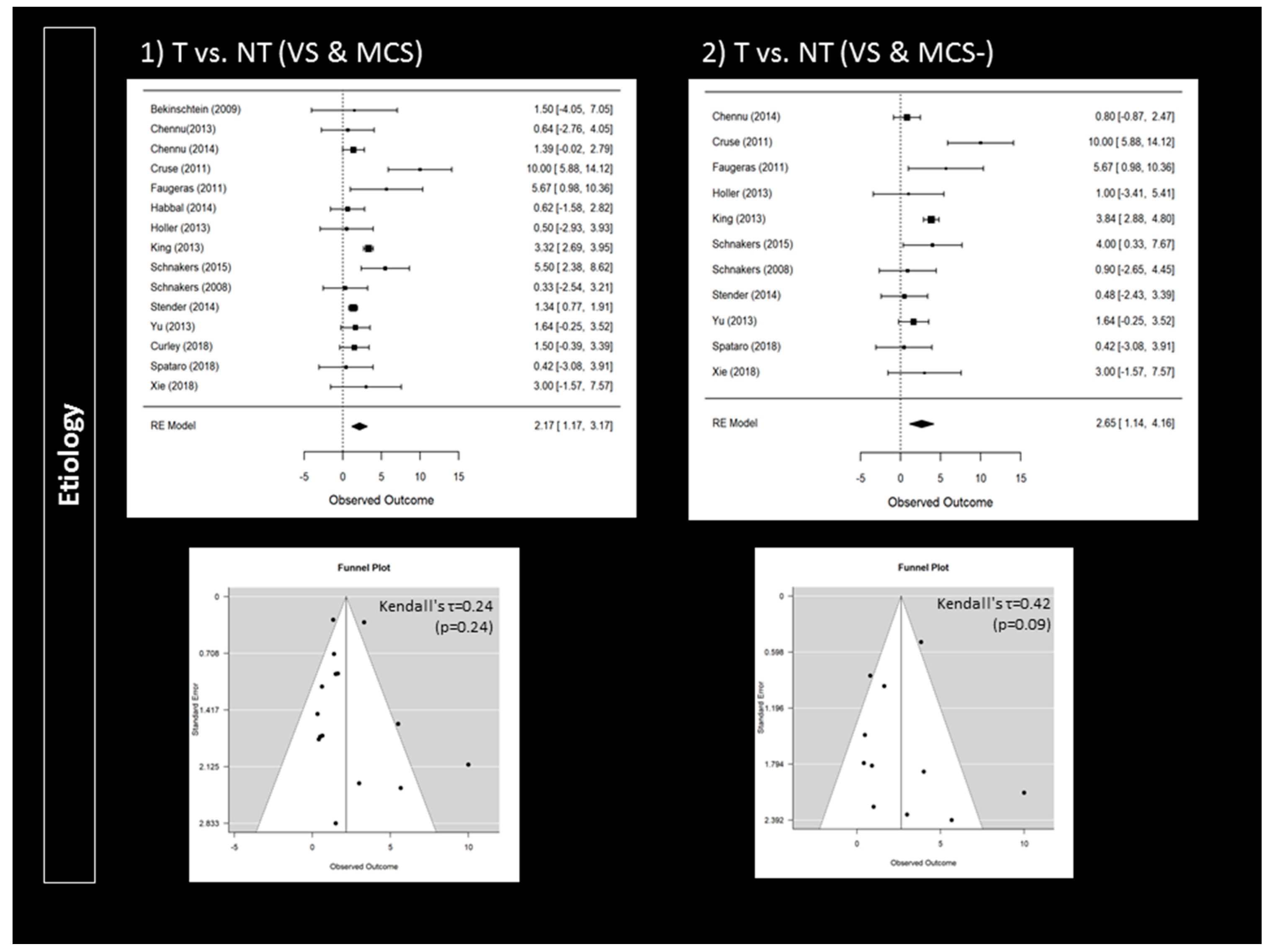
2.3. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The Multi-Society Task Force on Persistent Vegetative State. Medical aspects of the persistent vegetative state. NEJM 1994, 330, 1499–1508. [Google Scholar] [CrossRef]
- Giacino, J.; Ashwal, S.; Childs, N.; Cranford, R.; Jennett, B.; Katz, D.I.; Kelly, J.P.; Rosenberg, J.H.; Whyte, J.; Zafonte, R.D.; et al. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 58, 349–353. [Google Scholar] [CrossRef]
- Thibaut, A.; Bodien, Y.G.; Laureys, S.; Giacino, J.T. Minimally conscious state “plus”: Diagnostic criteria and relation to functional recovery. J. Neurol. 2020, 267, 1245–1254. [Google Scholar] [CrossRef]
- Wade, D.T. How often is the diagnosis of the permanent vegetative state incorrect? A review of the evidence. Eur. J. Neurol. 2018, 25, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Schnakers, C. Update on diagnosis in disorders of consciousness. Expert Rev. Neurother. 2020, 20, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. EAN Panel on Coma, Disorders of Consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Congress of Rehabilitation Medicine, Brain Injury-Interdisciplinary Special Interest Group. Assessment scales for disorders of consciousness: Evidence-based recommendations for clinical practice and research. Arch. Phys. Med. Rehabil. 2010, 91, 1795–1813. [Google Scholar] [CrossRef]
- Owen, A.M.; Coleman, M.R.; Boly, M.; Davis, M.H.; Laureys, S.; Pickard, J.D. Detecting awareness in the vegetative state. Science 2006, 313, 1402. [Google Scholar] [CrossRef] [Green Version]
- Monti, M.M.; Vanhaudenhuyse, A.; Coleman, M.R.; Boly, M.; Pickard, J.D.; Tshibanda, L.; Owen, A.M.; Laureys, S. Willful modulation of brain activity in disorders of consciousness. N. Engl. J. Med. 2010, 362, 579–589. [Google Scholar] [CrossRef] [Green Version]
- Owen, A.M. The Search for Consciousness. Neuron 2019, 102, 526–528. [Google Scholar] [CrossRef]
- Schiff, N.D. Cognitive Motor Dissociation Following Severe Brain Injuries. JAMA Neurol. 2015, 72, 1413–1415. [Google Scholar] [CrossRef]
- Kondziella, D.; Friberg, C.K.; Frokjaer, V.G.; Fabricius, M.; Møller, K. Preserved consciousness in vegetative and minimal conscious states: Systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 485–492. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice guideline update recommendations summary: Disorders of consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology 2018, 91, 450–460. [Google Scholar]
- Bekinschtein, T.A.; Dehaene, S.; Rohaut, B.; Tadel, F.; Cohen, L.; Naccache, L. Neural signature of the conscious processing of auditory regularities. Proc. Natl. Acad. Sci. USA 2009, 106, 1672–1677. [Google Scholar] [CrossRef] [Green Version]
- Chennu, S.; Finoia, P.; Kamau, E.; Monti, M.M.; Allanson, J.; Pickard, J.D.; Owen, A.M.; Bekinschtein, T.A. Dissociable endogenous and exogenous attention in disorders of consciousness. Neuroimage Clin. 2013, 3, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Chennu, S.; Finoia, P.; Kamau, E.; Allanson, J.; Williams, G.B.; Monti, M.M.; Noreika, V.; Arnatkeviciute, A.; Canales-Johnson, A.; Olivares, F.; et al. Spectral signatures of reorganised brain networks in disorders of consciousness. PLoS Comput. Biol. 2014, 10, e1003887. [Google Scholar] [CrossRef]
- Cruse, D.; Chennu, S.; Chatelle, C.; Bekinschtein, T.A.; Fernández-Espejo, D.; Pickard, J.D.; Laureys, S.; Owen, A.M. Bedside detection of awareness in the vegetative state: A cohort study. Lancet 2011, 378, 2088–2094. [Google Scholar] [CrossRef] [Green Version]
- Cruse, D.; Chennu, S.; Chatelle, C.; Fernández-Espejo, D.; Bekinschtein, T.A.; Pickard, J.D.; Laureys, S.; Owen, A.M. Relationship between etiology and covert cognition in the minimally conscious state. Neurology 2012, 78, 816–822. [Google Scholar] [CrossRef] [Green Version]
- Edlow, B.L.; Chatelle, C.; Spencer, C.A.; Chu, C.J.; Bodien, Y.G.; O’Connor, K.L.; Hirschberg, R.E.; Hochberg, L.R.; Giacino, J.T.; Rosenthal, E.S.; et al. Early detection of consciousness in patients with acute severe traumatic brain injury. Brain 2017, 140, 2399–2414. [Google Scholar] [CrossRef]
- Faugeras, F.; Rohaut, B.; Weiss, N.; Bekinschtein, T.A.; Galanaud, D.; Puybasset, L.; Bolgert, F.; Sergent, C.; Cohen, L.; Dehaene, S.; et al. Probing consciousness with event-related potentials in the vegetative state. Neurology 2011, 77, 264–268. [Google Scholar] [CrossRef] [Green Version]
- Gibson, R.M.; Fernández-Espejo, D.; Gonzalez-Lara, L.E.; Kwan, B.Y.; Lee, D.H.; Owen, A.M.; Cruse, D. Multiple tasks and neuroimaging modalities increase the likelihood of detecting covert awareness in patients with disorders of consciousness. Front. Hum. Neurosci. 2014, 8, 950. [Google Scholar] [CrossRef] [Green Version]
- Habbal, D.; Gosseries, O.; Noirhomme, Q.; Renaux, J.; Lesenfants, D.; Bekinschtein, T.A.; Majerus, S.; Laureys, S.; Schnakers, C. Volitional electromyographic responses in disorders of consciousness. Brain Inj. 2014, 28, 1171–1179. [Google Scholar] [CrossRef] [Green Version]
- Hauger, S.L.; Schnakers, C.; Andersson, S.; Becker, F.; Moberget, T.; Giacino, J.T.; Schanke, A.K.; Løvstad, M. Neurophysiological Indicators of Residual Cognitive Capacity in the Minimally Conscious State. Behav. Neurol. 2015, 2015, 145913. [Google Scholar] [CrossRef] [Green Version]
- Hauger, S.L.; Schanke, A.K.; Andersson, S.; Chatelle, C.; Schnakers, C.; Løvstad, M. The Clinical Diagnostic Utility of Electrophysiological Techniques in Assessment of Patients with Disorders of Consciousness Following Acquired Brain Injury: A Systematic Review. J. Head Trauma Rehabil. 2017, 32, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Höller, Y.; Bergmann, J.; Thomschewski, A.; Kronbichler, M.; Höller, P.; Crone, J.S.; Schmid, E.V.; Butz, K.; Nardone, R.; Trinka, E. Comparison of EEG-features and classification methods for motor imagery in patients with disorders of consciousness. PLoS ONE 2013, 8, e80479. [Google Scholar] [CrossRef] [Green Version]
- King, J.R.; Faugeras, F.; Gramfort, A.; Schurger, A.; El Karoui, I.; Sitt, J.D.; Rohaut, B.; Wacongne, C.; Labyt, E.; Bekinschtein, T.; et al. Single-trial decoding of auditory novelty responses facilitates the detection of residual consciousness. Neuroimage 2013, 83, 726–738. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Pan, J.; He, Y.; Wang, F.; Laureys, S.; Xie, Q.; Yu, R. Detecting number processing and mental calculation in patients with disorders of consciousness using a hybrid brain-computer interface system. BMC Neurol. 2015, 15, 259. [Google Scholar] [CrossRef] [Green Version]
- Schnakers, C.; Giacino, J.T.; Løvstad, M.; Habbal, D.; Boly, M.; Di, H.; Majerus, S.; Laureys, S. Preserved covert cognition in noncommunicative patients with severe brain injury? Neurorehabil. Neural Repair 2015, 29, 308–317. [Google Scholar] [CrossRef]
- Schnakers, C.; Perrin, F.; Schabus, M.; Majerus, S.; Ledoux, D.; Damas, P.; Boly, M.; Vanhaudenhuyse, A.; Bruno, M.A.; Moonen, G.; et al. Voluntary brain processing in disorders of consciousness. Neurology 2008, 71, 1614–1620. [Google Scholar] [CrossRef] [Green Version]
- Stender, J.; Gosseries, O.; Bruno, M.A.; Charland-Verville, V.; Vanhaudenhuyse, A.; Demertzi, A.; Chatelle, C.; Thonnard, M.; Thibaut, A.; Heine, L.; et al. Diagnostic precision of PET imaging and functional MRI in disorders of consciousness: A clinical validation study. Lancet 2014, 384, 514–522. [Google Scholar] [CrossRef]
- Vogel, D.; Markl, A.; Yu, T.; Kotchoubey, B.; Lang, S.; Müller, F. Can mental imagery functional magnetic resonance imaging predict recovery in patients with disorders of consciousness? Arch. Phys. Med. Rehabil. 2013, 94, 1891–1898. [Google Scholar] [CrossRef]
- Wang, F.; He, Y.; Pan, J.; Xie, Q.; Yu, R.; Zhang, R.; Li, Y. A Novel Audiovisual Brain-Computer Interface and Its Application in Awareness Detection. Sci. Rep. 2015, 5, 9962. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Lang, S.; Vogel, D.; Markl, A.; Müller, F.; Kotchoubey, B. Patients with unresponsive wakefulness syndrome respond to the pain cries of other people. Neurology 2013, 80, 345–352. [Google Scholar] [CrossRef]
- Chatelle, C.; Spencer, C.A.; Cash, S.S.; Hochberg, L.R.; Edlow, B.L. Feasibility of an EEG-based brain-computer interface in the intensive care unit. Clin. Neurophysiol. 2018, 129, 1519–1525. [Google Scholar] [CrossRef]
- Curley, W.H.; Forgacs, P.B.; Voss, H.U.; Conte, M.M.; Schiff, N.D. Characterization of EEG signals revealing covert cognition in the injured brain. Brain 2018, 141, 1404–1421. [Google Scholar] [CrossRef]
- Spataro, R.; Heilinger, A.; Allison, B.; De Cicco, D.; Marchese, S.; Gregoretti, C.; La Bella, V.; Guger, C. Preserved somatosensory discrimination predicts consciousness recovery in unresponsive wakefulness syndrome. Clin. Neurophysiol. 2018, 129, 1130–1136. [Google Scholar] [CrossRef]
- Xie, Q.; Pan, J.; Chen, Y.; He, Y.; Ni, X.; Zhang, J.; Wang, F.; Li, Y.; Yu, R. A gaze-independent audiovisual brain-computer Interface for detecting awareness of patients with disorders of consciousness. BMC Neurol. 2018, 18, 144. [Google Scholar] [CrossRef]
- Aubinet, C.; Murphy, L.; Bahri, M.A.; Larroque, S.K.; Cassol, H.; Annen, J.; Carrière, M.; Wannez, S.; Thibaut, A.; Laureys, S.; et al. Brain, Behavior, and Cognitive Interplay in Disorders of Consciousness: A Multiple Case Study. Front. Neurol. 2018, 9, 665. [Google Scholar] [CrossRef]
- Aubinet, C.; Larroque, S.K.; Heine, L.; Martial, C.; Majerus, S.; Laureys, S.; Di Perri, C. Clinical subcategorization of minimally conscious state according to resting functional connectivity. Hum. Brain Mapp. 2018, 39, 4519–4532. [Google Scholar] [CrossRef] [Green Version]
- Aubinet, C.; Cassol, H.; Gosseries, O.; Bahri, M.A.; Larroque, S.K.; Majerus, S.; Martial, C.; Martens, G.; Carrière, M.; Chatelle, C.; et al. Brain Metabolism but Not Gray Matter Volume Underlies the Presence of Language Function in the Minimally Conscious State (MCS): MCS+ Versus MCS- Neuroimaging Differences. Neurorehabil. Neural Repair 2020, 34, 172–184. [Google Scholar] [CrossRef]
- Fernández-Espejo, D.; Rossit, S.; Owen, A.M. A Thalamocortical Mechanism for the Absence of Overt Motor Behavior in Covertly Aware Patients. JAMA Neurol. 2015, 72, 1442–1450. [Google Scholar] [CrossRef] [Green Version]
- Schnakers, C.; Monti, M.M. Disorders of consciousness after severe brain injury: Therapeutic options. Curr. Opin. Neurol. 2017, 30, 573–579. [Google Scholar] [CrossRef]
- Pignat, J.M.; Mauron, E.; Jöhr, J.; Gilart de Keranflech, C.; Van De Ville, D.; Preti, M.G.; Meskaldji, D.E.; Hömberg, V.; Laureys, S.; Draganski, B.; et al. Outcome Prediction of Consciousness Disorders in the Acute Stage Based on a Complementary Motor Behavioural Tool. PLoS ONE 2016, 11, e0156882. [Google Scholar] [CrossRef]
- Pincherle, A.; Jöhr, J.; Chatelle, C.; Pignat, J.M.; Du Pasquier, R.; Ryvlin, P.; Oddo, M.; Diserens, K. Motor behavior unmasks residual cognition in disorders of consciousness. Ann. Neurol. 2019, 85, 443–447. [Google Scholar] [CrossRef]
- Pincherle, A.; Rossi, F.; Jöhr, J.; Dunet, V.; Ryvlin, P.; Oddo, M.; Schiff, N.; Diserens, K. Early discrimination of cognitive motor dissociation from disorders of consciousness: Pitfalls and clues. J. Neurol. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| ARTICLE | Risks of BIAS | APPLICABILITY Concerns | Paradigm | Modality | Responders |
|---|---|---|---|---|---|
| Bekinschtein (2009) [17] | HIGH | LOW | Local-global effect (count) | fMRI/EEG | 28.57% |
| Chennu (2013) [18] | HIGH | LOW | Local-global effect (count) | fMRI/EEG | 19.05% |
| Chennu (2014) [19] | HIGH | LOW | Local-global effect (count) | EEG | 43.33% |
| Cruse (2011) [20] | LOW | LOW | Motor imagery | EEG | 20.00% |
| Cruse (2012) [21] | HIGH | LOW | Motor imagery | EEG | 21.05% |
| Edlow (2017) [22] | LOW | HIGH | Motor imagery | fMRI/EEG | 43.75% |
| Faugeras (2011) [23] | HIGH | LOW | Count target | EEG | 9.09% |
| Gibson (2014) [24] | HIGH | LOW | Spatial and motor imagery | fMRI/EEG | 66.67% |
| Habbal (2014) [25] | LOW | LOW | Motor imagery | EMG | 10.53% |
| Hauger (2015) [26] | HIGH | LOW | Count target | EEG | 10.00% |
| Hauger (2017) [27] | HIGH | LOW | Count target | EEG | 62.50% |
| Holler (2013) [28] | HIGH | LOW | Motor imagery | EEG | 35.71% |
| King (2013) [29] | HIGH | LOW | Count target | EEG | 26.14% |
| Li (2015) [30] | HIGH | LOW | Mental calculation | EEG | 33.33% |
| Monti (2010) [9] | HIGH | LOW | Spatial and motor imagery | fMRI | 7.69% |
| Schnakers (2015) [31] | LOW | LOW | Focus attention | EEG | 19.05% |
| Schnakers (2008) [32] | LOW | LOW | Count target | EEG | 27.27% |
| Stender (2014) [33] | HIGH | LOW | Spatial and motor imagery | fMRI | 33.33% |
| Vogel (2013) [34] | HIGH | LOW | Spatial and motor imagery | fMRI | 60.00% |
| Wang (2015) [35] | HIGH | LOW | Count target | EEG | 71.43% |
| Yu (2013) [36] | HIGH | LOW | Count target | fMRI | 11.63% |
| Chatelle (2018) [37] | LOW | HIGH | Count and motor imagery | EEG | 40.00% |
| Curley (2018) [38] | LOW | LOW | Motor imagery | fMRI/EEG | 34.78% |
| Spataro (2018) [39] | HIGH | LOW | Count target | EEG | 30.77% |
| Xie (2018) [40] | HIGH | LOW | Focus attention | EEG | 37.50% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnakers, C.; Hirsch, M.; Noé, E.; Llorens, R.; Lejeune, N.; Veeramuthu, V.; De Marco, S.; Demertzi, A.; Duclos, C.; Morrissey, A.-M.; et al. Covert Cognition in Disorders of Consciousness: A Meta-Analysis. Brain Sci. 2020, 10, 930. https://doi.org/10.3390/brainsci10120930
Schnakers C, Hirsch M, Noé E, Llorens R, Lejeune N, Veeramuthu V, De Marco S, Demertzi A, Duclos C, Morrissey A-M, et al. Covert Cognition in Disorders of Consciousness: A Meta-Analysis. Brain Sciences. 2020; 10(12):930. https://doi.org/10.3390/brainsci10120930
Chicago/Turabian StyleSchnakers, Caroline, Michaela Hirsch, Enrique Noé, Roberto Llorens, Nicolas Lejeune, Vigneswaran Veeramuthu, Sabrina De Marco, Athena Demertzi, Catherine Duclos, Ann-Marie Morrissey, and et al. 2020. "Covert Cognition in Disorders of Consciousness: A Meta-Analysis" Brain Sciences 10, no. 12: 930. https://doi.org/10.3390/brainsci10120930