
Cross-Cultural Adaptation and Evaluation of the Participation and Environment Measure for Children and Youth to the Indian Context—A Mixed-Methods Study


Abstract
:1. Introduction
Objectives
2. Materials and Methods
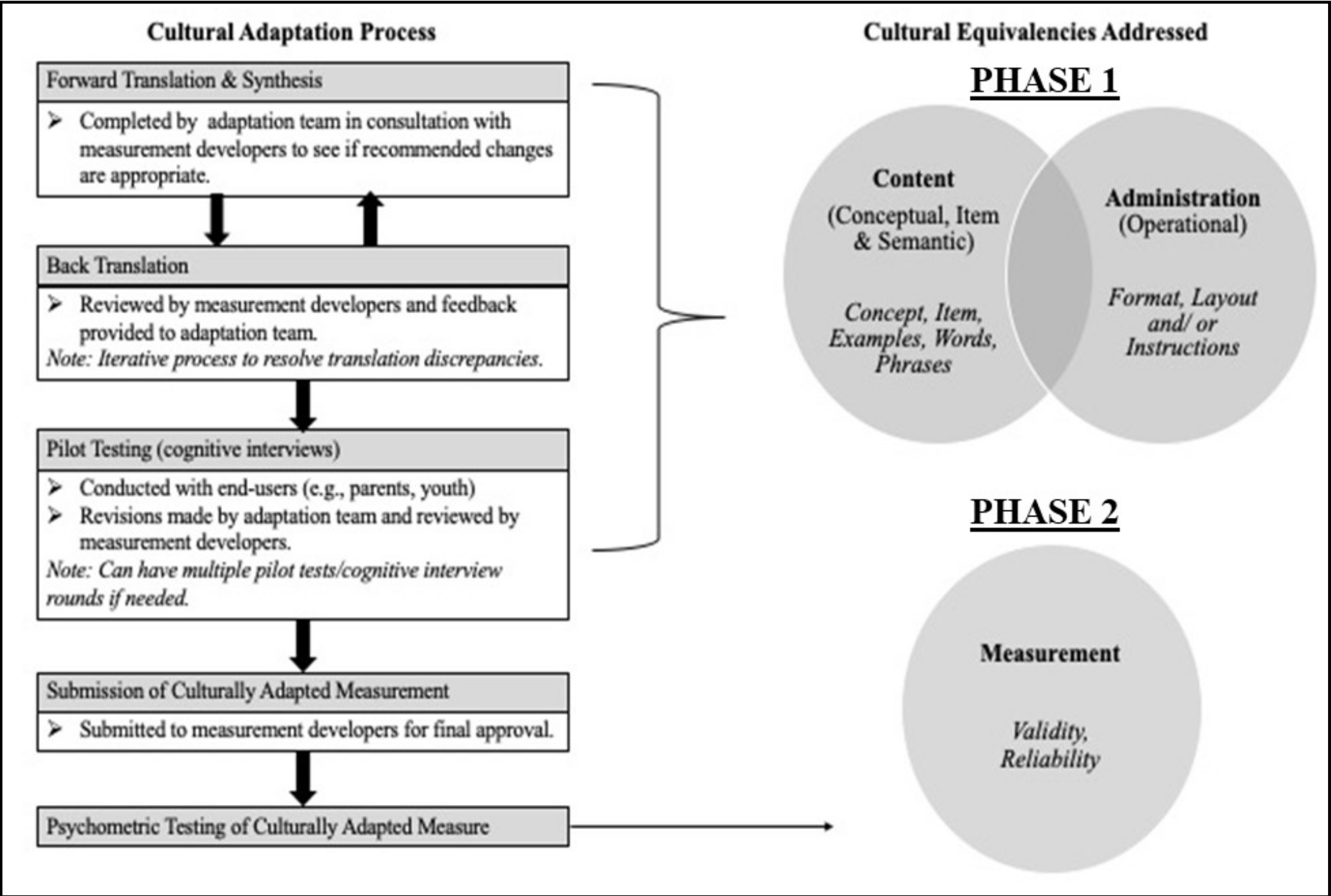
2.1. Study Design
2.2. Procedure
2.3. Measurements
2.4. Data Analysis
3. Results
3.1. Phase 1—Caregiver and Child Characteristics
Modifications in English and Hindi PEM-CY
- Clarifying Survey Instructions included providing explanations for concepts such as “involvement” and pictorial examples for completing the participation and environment sections. A sample of a completed PEM-CY question with clear instructions for entering responses was added to the survey instructions (see Figure 2). Specific pointers such as “For question B on Involvement” were used instead of the less specific term “important” that was part of the original survey instructions. The stem questions and response options were elaborated and made more self-explanatory after Round 2. For example, the question “What do you do to support your child’s participation?” was modified to “What do you do to support your child’s participation at present?” to make the question easier to understand and respond to. Contextually relatable examples were used for environmental supports that could be made available to enhance the child’s participation (e.g., In the survey guidelines-wheelchair to support mobility was used as an example of environmental support).
- Reformatting of the questionnaire was also required. Specifically, modifications such as increased font size, color coding, italicizing, underlining, the spacing between items, and columns were used to draw the attention of the caregiver to important instructions and steps in both rounds of interviews.
- Help with transitions within the PEM-CY sections was also needed. Transition boxes were added between the participation and environment section to alert the caregiver to the change in section.
3.2. Phase 2
3.2.1. Caregiver Characteristics (n = 130)
3.2.2. Psychometric Properties
Construct Validity of the Adapted PEM-CY
Reliability of the Adapted PEM-CY
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Level of Assistance | Type of Assistance |
|---|---|
| Level 1 | Redirecting them to the survey guidelines (Formatting issues, reminding to reread survey guidelines). |
| Level 2 | Prompts like reading out the items and asking questions like “what opportunities are available in your context?” (reading with them and encouraging them to think of examples related to their context). |
| Level 3 | Discussion over an item and then filling up the question (explaining the item to them, giving them examples, talking about understanding, and relating to their context). |
References
- Law, M. Participation in the Occupations of Everyday Life. Am. J. Occup. Ther. 2002, 640–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF. Int. Classif. 2002, 1149, 1–22. [Google Scholar]
- World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF). Exposure Draft for Comment; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Law, M.; Anaby, D.; Teplicky, R.; Khetani, M.A.; Coster, W.; Bedell, G. Participation in the Home Environment among Children and Youth with and without Disabilities. Br. J. Occup. Ther. 2013, 76, 58–66. [Google Scholar] [CrossRef]
- Imms, C.; Adair, B.; Keen, D.; Ullenhag, A.; Rosenbaum, P.; Granlund, M. “Participation”: A Systematic Review of Language, Definitions, and Constructs Used in Intervention Research with Children with Disabilities. Dev. Med. Child Neurol. 2016, 58, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Coster, W.; Bedell, G.; Law, M.; Khetani, M.A.; Teplicky, R.; Liljenquist, K.; Gleason, K.; Kao, Y.C. Psychometric Evaluation of the Participation and Environment Measure for Children and Youth. Dev. Med. Child Neurol. 2011, 53, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Adair, B.; Ullenhag, A.; Rosenbaum, P.; Granlund, M.; Keen, D.; Imms, C. Measures Used to Quantify Participation in Childhood Disability and Their Alignment with the Family of Participation-Related Constructs: A Systematic Review. Dev. Med. Child Neurol. 2018, 60, 1101–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resch, C.; Van Kruijsbergen, M.; Ketelaar, M.; Hurks, P.; Adair, B.; Imms, C.; De Kloet, A.; Piskur, B.; Van Heugten, C. Assessing Participation of Children with Acquired Brain Injury and Cerebral Palsy: A Systematic Review of Measurement Properties. Dev. Med. Child Neurol. 2020, 62, 434–444. [Google Scholar] [CrossRef]
- Bedell, G.M.; Khetani, M.A.; Cousins, M.A.; Coster, W.J.; Law, M.C. Parent Perspectives to Inform Development of Measures of Children’s Participation and Environment. Arch. Phys. Med. Rehabil. 2011, 92, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Khetani, M. Psychometric Evaluation of the Young Children’s Participation and Environment Measure (YC–PEM). Am. J. Occup. Ther. 2015, 69, 6911500184p1. [Google Scholar] [CrossRef]
- Olusanya, B.O.; Davis, A.C.; Wertlieb, D.; Boo, N.Y.; Nair, M.K.C.; Halpern, R.; Kuper, H.; Breinbauer, C.; de Vries, P.J.; Gladstone, M.; et al. Developmental Disabilities among Children Younger than 5 Years in 195 Countries and Territories, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Glob. Health 2018, 6, e1100–e1121. [Google Scholar] [CrossRef] [Green Version]
- Schlebusch, L.; Huus, K.; Samuels, A.; Granlund, M.; Dada, S. Participation of Young People with Disabilities and/or Chronic Conditions in Low- and Middle-Income Countries: A Scoping Review. Dev. Med. Child Neurol. 2020, 62, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Dada, S.; Bastable, K.; Halder, S. The Role of Social Support in Participation Perspectives of Caregivers of Children with Intellectual Disabilities in India and South Africa. Int. J. Environ. Res. Public Health 2020, 17, 6644. [Google Scholar] [CrossRef] [PubMed]
- Jindal, P.; MacDermid, J.C.; Rosenbaum, P.; DiRezze, B.; Narayan, A. Perspectives on Rehabilitation of Children with Cerebral Palsy: Exploring a Cross-Cultural View of Parents from India and Canada Using the International Classification of Functioning, Disability and Health. Disabil. Rehabil. 2018, 40, 2745–2755. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.G.; Roy, G.; Kar, S.S. Disability and Rehabilitation Services in India: Issues and Challenges. J. Fam. Med. Prim. care 2012, 1, 69–73. [Google Scholar] [CrossRef]
- Creswell, J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2014; Volume 71. [Google Scholar] [CrossRef]
- Lim, C.Y.; Law, M.; Khetani, M.; Pollock, N.; Rosenbaum, P. Establishing the Cultural Equivalence of the Young Children’s Participation and Environment Measure (YC-PEM) for Use in Singapore. Phys. Occup. Ther. Pediatr. 2016, 36, 422–439. [Google Scholar] [CrossRef] [Green Version]
- Stevelink, S.A.M.; Van Brakel, W.H. The Cross-Cultural Equivalence of Participation Instruments: A Systematic Review. Disabil. Rehabil. 2013, 35, 1256–1268. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality Criteria Were Proposed for Measurement Properties of Health Status Questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Tomas, V.; Srinivasan, R.; Kulkarni, V.; Teplicky, R.; Anaby, D.; Khetani, M. A Guiding Process for Culturally Adapting Assessments for Participation-Focused Pediatric Practice: The Case of the Participation and Environment Measures (PEM). Disabil. Rehabil. 2020. Under review. [Google Scholar]
- Beaton, D.E.; Claire, B.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 1976, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Bowden, A.; Fox-Rushby, J.A. A Systematic and Critical Review of the Process of Translation and Adaptation of Generic Health-Related Quality of Life Measures in Africa, Asia, Eastern Europe, the Middle East, South America. Soc. Sci. Med. 2003, 57, 1289–1306. [Google Scholar] [CrossRef]
- Peterson, C.H.; Peterson, N.A.; Powell, K.G. Cognitive Interviewing for Item Development: Validity Evidence Based on Content and Response Processes. Meas. Eval. Couns. Dev. 2017, 50, 217–223. [Google Scholar] [CrossRef]
- Patrick, D.L.; Burke, L.B.; Gwaltney, C.J.; Leidy, N.K.; Martin, M.L.; Molsen, E.; Ring, L. Content Validity-Establishing and Reporting the Evidence in Newly Developed Patient-Reported Outcomes (PRO) Instruments for Medical Product Evaluation: ISPOR PRO Good Research Practices Task Force Report: Part 2-Assessing Respondent Understanding. Value Health 2011, 14, 978–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charters, E. The Use of Think-Aloud Methods in Qualitative Research An Introduction to Think-Aloud Methods. Brock Educ. J. 2003, 12. [Google Scholar] [CrossRef]
- Chow, S.C.; Shao, J.; Wang, H. Sample Size Calculations in Clinical Research, 2nd ed.; Chapman & Hall: New York, NY, USA, 2008. [Google Scholar]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use, 5th ed.; Oxford University Press: Oxford, UK, 2008. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Anaby, D.; Khetani, M.; Teplicky, R. PEM-CY User’s Guide; Version 1.1; CanChild Centre for Childhood Disability Research McMaster University: Hamilton, ON, Canada, 2014. [Google Scholar]
- McCormack, H.M.; Horne, D.J.d.L.; Sheather, S. Clinical Applications of Visual Analogue Scales: A Critical Review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef] [PubMed]
- Paul-Dauphin, A.; Guillemin, F.; Virion, J.M.; Briançon, S. Bias and Precision in Visual Analogue Scales: A Randomized Controlled Trial. Am. J. Epidemiol. 1999, 150, 1117–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anaby, D.; Law, M.; Coster, W.; Bedell, G.; Khetani, M.; Avery, L.; Teplicky, R. The Mediating Role of the Environment in Explaining Participation of Children and Youth with and without Disabilities across Home, School, and Community. Arch. Phys. Med. Rehabil. 2014, 95, 908–917. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Knafl, K.; Deatrick, J.; Gallo, A.; Holcombe, G.; Bakitas, M.; Dixon, J.; Grey, M. The Analysis and Interpretation of Cognitive Interviews for Instrument Development. Res. Nurs. Health 2007, 30, 224–234. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; De Vet, H.C. The COSMIN Checklist for Evaluating the Methodological Quality of Studies on Measurement Properties: A Clarification of Its Content. BMC Med. Res. Methodol. 2010, 10. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, A.S.S.; Wilk, M.B. An Analysis of Variance Test for Normality. Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. Landis Amd Koch1977_agreement of Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 2nd ed.; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Munyi, C.W. Past and Present Perceptions Towards Disability: A Historical Perspective. Disabil. Stud. Q. 2012, 32. [Google Scholar] [CrossRef]
- Krieger, B.; Schulze, C.; Boyd, J.; Amann, R.; Piškur, B.; Beurskens, A.; Teplicky, R.; Moser, A. Cross-Cultural Adaptation of the Participation and Environment Measure for Children and Youth (PEM-CY) into German: A Qualitative Study in Three Countries. BMC Pediatr. 2020, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.; Law, M.; Stratford, P.; DeMatteo, C.; Kim, H. Cross-Cultural Validation and Psychometric Evaluation of the Participation and Environment Measure for Children and Youth in Korea. Disabil. Rehabil. 2016, 38, 2217–2228. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health Literacy as a Public Health Goal: A Challenge for Contemporary Health Education and Communication Strategies into the 21st Century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]


| Equivalence Criteria | Definition of Criteria | |
|---|---|---|
| Phase1: Qualitative focus | Conceptual | The relevance of the underlying domain |
| Item | Acceptability of items | |
| Semantic | Consistency of the meaning in the local language | |
| Operational | Suitability of instructions, administration, formatting, design | |
| Phase 2: Quantitative focus | Measurement | Equivalence in the psychometric properties |
| Round 1 (n = 10) | Round 2 (n = 5) | |
|---|---|---|
| Caregivers | ||
| Fathers | 1 | 1 |
| Mothers | 9 | 4 |
| Caregiver education | ||
| Up to High school | 2 | 5 |
| Graduation | 6 | 0 |
| Postgraduation | 2 | 0 |
| Employment status | ||
| Employed | 4 | 2 |
| Unemployed | 6 | 3 |
| Monthly Family Income | ||
| Below Minimum Wage (INR 10,000) | 2 | 3 |
| Above Minimum Wage (INR 10,000) | 8 | 2 |
| Children | ||
| Sex | ||
| Males | 7 | 3 |
| Females | 3 | 2 |
| Age | ||
| 5–8 years | 7 | 1 |
| 8.1–12 years | 2 | 4 |
| 12.1–17 years | 1 | 0 |
| Diagnosis | ||
| Autism Spectrum Disorder | 3 | 0 |
| Autism Spectrum Disorder and Global Developmental Delay | 1 | 0 |
| Autism Spectrum Disorder and Intellectual Disability | 1 | 0 |
| Cerebral Palsy | 1 | 0 |
| Cerebral Palsy with Global Developmental Delay, Vision Impairment and Hearing Impairment | 0 | 1 |
| Global Developmental Delay | 0 | 1 |
| Global Developmental Delay and Learning Disability | 1 | 0 |
| Global Developmental Delay and Cerebral Palsy | 1 | 0 |
| Attention Deficit Hyperactivity Disorder | 1 | 0 |
| Language Disorder | 1 | 0 |
| Learning Disability | 0 | 2 |
| Intellectual Disability | 0 | 1 |
| Variable | Cases (n = 65) n% | Controls (n = 65) n% | ||
|---|---|---|---|---|
| Child Gender | ||||
| Male | 37 | 57% | 40 | 62% |
| Female | 28 | 43% | 25 | 38% |
| Child Age (Mean = 8.7 years) | ||||
| 5–8 | 27 | 42% | 27 | 41% |
| 8.1–12 | 21 | 32% | 21 | 32% |
| 12.1–15 | 15 | 23% | 13 | 20% |
| 15.1 to 18 | 2 | 3% | 4 | 6% |
| Autism Spectrum Disorder | 21 | 32% | - | - |
| Specific Learning Disability | 17 | 26% | - | - |
| Attention Deficit Hyperactivity Disorder | 16 | 25% | - | - |
| Global Developmental Delay | 16 | 25% | - | - |
| Child—Number of health conditions | ||||
| 1 | 30 | 46% | - | - |
| 2 | 11 | 17% | - | - |
| 3 | 18 | 28% | - | - |
| 0 | 6 | 9% | - | - |
| Child—Number of functional limitations | ||||
| 1–3 | 16 | 25% | - | - |
| 4–6 | 26 | 40% | - | - |
| 7–9 | 19 | 29% | - | - |
| 10–11 | 4 | 6% | - | - |
| Respondent relationship to the child | ||||
| Mother | 49 | 75% | 55 | 85% |
| Father | 16 | 25% | 6 | 9% |
| Other | 0 | 0% | 4 | 6% |
| Respondent age (years) | ||||
| 18–29 | 3 | 5% | 9 | 14% |
| 30–39 | 36 | 55% | 35 | 53% |
| 40–55 | 24 | 37% | 20 | 31% |
| Missing | 2 | 3% | 1 | 2% |
| Respondent education | ||||
| High School Education or lower | 26 | 40% | 26 | 40% |
| Graduate/Diploma/technical training | 25 | 38% | 27 | 42% |
| Postgraduate | 14 | 22% | 12 | 18% |
| Family income * | ||||
| Above Minimum Wage (INR 10,000/136.5 USD) | 47 | 72% | 50 | 76.9% |
| Below Minimum Wage (INR 10,000/136.5 USD) | 17 | 26% | 10 | 15.3% |
| Language of PEM-CY | ||||
| English | 32 | 49% | 37 | 57% |
| Hindi | 33 | 51% | 28 | 43% |
| . | Cases (n = 65) | Controls (n = 65) | n = 130 | n = 130 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Home | ||||||||||
| Min | Max | Mean | Sd | Mean | Sd | Z/T value * | p-value | Internal consistency (Cronbach’s alpha) | Effect size (Cohen’s d) | |
| Average frequency of home Participation | 4.17 | 7 | 6.05 | 0.63 | 6.32 | 0.54 | −2.649 | 0.008 | 0.7103 | 0.5759 |
| Percentage of activities at home | 10% | 100% | 87.23% | 19.73% | 92.92% | 9.14% | −0.939 | 0.347 | 0.2419 | |
| Average of involvements at home | 1 | 5 | 3.56 | 0.79 | 4.04 | 0.74 | −3.716 | <0.001 | 0.7158 | 0.7036 |
| Home-percentage of change desired | 0% | 100% | 77.28% | 25.89% | 54.91% | 27.77% | −4.613 | <<0.001 | 0.8161 | 0.8157 |
| Home environment-score 3 (Support) | 0 | 66.7% | 27.692% | 16.345% | 32.692% | 18.768% | −1.695 | 0.090 | 0.8303 | 1.2377 (HE) |
| Home environment-score 1 (Barriers) | 0 | 66.6% | 16.154% | 16.853% | 2.820% | 6.633% | −5.837 | <<0.001 | ||
| School | ||||||||||
| Min | Max | Mean | Sd | Mean | Sd | Z/T value * | p-value | Internal consistency (Cronbach’s alpha) | Effect size (Cohen’s d) | |
| Average of school frequency ** | 1 | 7 | 4.73 | 1.32 (IQR: 1.70) | 5.42 | 1.00 (IQR: 1.65) | −3.272 | 0.0013 | 0.6079 | 0.9225 |
| Percentage of activities at school | 20% | 100% | 68% | 26% | 83% | 20% | −3.257 | 0.001 | 0.3038 | |
| Average of involvements at school | 1 | 5 | 3.12 | 1.28 | 4.11 | 0.86 | −4.457 | <<0.001 | 0.7041 | 0.871 |
| School percentage of change desired | 0 | 100 | 78.65% | 30.86% | 45.47% | 38.25% | −4.960 | <<0.001 | 0.8535 | 1.0339 |
| School environment-score 3 (Support) | 0 | 94% | 35.93% | 21.57% | 39.71% | 18.98% | −1.195 | 0.232 | 0.8647 | 1.1139 (SE) |
| School environment-score 1 (Barriers) | 0 | 70.5% | 15.20% | 19.28% | 2.85% | 5.55% | −4.618 | <<0.001 | ||
| Community | ||||||||||
| Min | Max | Mean | Sd | Mean | Sd | Z/T value * | p-value | Internal consistency (Cronbach’s alpha) | Effect size (Cohen’s d) | |
| Average of community frequency ** | 1.83 | 6.80 | 4.27 | 1.07 (IQR: 1.47) | 4.81 | 1.17 (IQR: 1.44) | −2.724 | 0.0073 | 0.7355 | 0.8076 |
| Percentage of activities at community | 0 | 10% | 54% | 21% | 66% | 19% | −3.486 | <0.001 | 0.0543 | |
| Average of involvements at community | 1 | 5 | 3.13 | 1.12 | 3.87 | 0.91 | −3.486 | <0.001 | 0.7929 | 0.525 |
| Community percentage of change desired | 0 | 100% | 73.18% | 28.98% | 49.74% | 34.00% | −4.006 | <<0.001 | 0.8626 | 0.7774 |
| Community environment-score 3 (Support) | 0 | 93.7% | 28.17% | 18.95% | 30.19% | 18.51% | −0.710 | 0.478 | 0.8768 | 1.0235 (CE) |
| Community environment-score 1 (Barriers) | 0 | 81.25% | 21.83% | 22.78% | 8.56% | 13.05% | −3.876 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srinivasan, R.; Kulkarni, V.; Smriti, S.; Teplicky, R.; Anaby, D. Cross-Cultural Adaptation and Evaluation of the Participation and Environment Measure for Children and Youth to the Indian Context—A Mixed-Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 1514. https://doi.org/10.3390/ijerph18041514
Srinivasan R, Kulkarni V, Smriti S, Teplicky R, Anaby D. Cross-Cultural Adaptation and Evaluation of the Participation and Environment Measure for Children and Youth to the Indian Context—A Mixed-Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1514. https://doi.org/10.3390/ijerph18041514
Chicago/Turabian StyleSrinivasan, Roopa, Vrushali Kulkarni, Sana Smriti, Rachel Teplicky, and Dana Anaby. 2021. "Cross-Cultural Adaptation and Evaluation of the Participation and Environment Measure for Children and Youth to the Indian Context—A Mixed-Methods Study" International Journal of Environmental Research and Public Health 18, no. 4: 1514. https://doi.org/10.3390/ijerph18041514